AUCTORES
Globalize your Research

Review Article | DOI: https://doi.org/10.31579/2692-9406/082
*Corresponding Author: Li Zhong, College of Osteopathic Medicine of the Pacific, Western University of Health Sciences, Pomona, California 91766, USA.
Citation: J Ly, Q Chu and L Zhong. (2021) Novel Therapeutic Trends in Pneumonia: Antibiotics and Mesenchymal Stem Cells. Biomedical Research and Clinical Reviews. 4(5); DOI: 10.31579/2692-9406/082
Copyright: © 2021 Li Zhong, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 24 August 2021 | Accepted: 13 September 2021 | Published: 20 September 2021
Keywords: community-acquired pneumonia; hospital-acquired pneumonia; antibiotics; mesenchymal stem cells; corticosteroids; COVID-19
Pneumonia remains a major cause of morbidity and mortality. With the significant global health burden that pneumonia poses, it is essential to improve therapeutic and management strategies. The increasing emergence of antibiotic-resistant bacterial strains limits options for effective antibiotic use. New antibiotics for the treatment of pneumonia may address deficits in current antimicrobial drugs, with an ability to cover both typical, atypical, and resistant pathogens. Several of these newer drugs also have structural characteristics that allow for a decreased propensity for the development of bacterial resistance. The potential use of stem cell therapies in place of corticosteroid treatments may also offer an improvement in patient outcomes. Human mesenchymal stem cell treatments have shown efficacy and safety in treating COVID-19 induced pneumonia. Combined treatment with both stem cells and antibiotics in pneumonia in a rabbit model has also shown significantly increased efficacy in comparison to antibiotic treatment alone. This presents yet another possible route for a novel strategy in treating pneumonia, though additional future studies are necessary before clinical implementation. While pneumonia remains a major disease of concern, having newer approved antibiotics as well as novel therapies such as stem cell treatments in the pipeline offers clinicians more options in effectively treating pneumonia.
Pneumonia, defined as an infection of the lung or pulmonary parenchyma by bacteria, viruses, fungi, and/or bacteria-like organisms, is one of the leading causes of morbidity and mortality globally [1-3]. Pneumonia is characterized by symptoms including fever, sweating, shortness of breath, chest pain, fatigue and loss of appetite [1]. The most common pneumonia is community-acquired pneumonia (CAP), which is pneumonia acquired outside of a hospital setting [3]. S. pneumoniae, H. influenzae, S. aureus, and the influenza virus, are the main causative agents of CAP, with S. pneumoniae accounting for more than 25% of cases of CAP worldwide [1,3,4]. Hospital-acquired pneumonia (HAP), another common form of pneumonia, is acquired after at least 48 hours of hospitalization for other diseases [1,3]. While HAP can be caused by gram-positive cocci such as S. aureus and S. pneumoniae, gram-negative bacilli such as P. aeruginosa, K. pneumoniae, E. coli, and Enterobacter are more likely to be involved in HAP [1].
CAP has been shown to greatly increase the risk of long-term morbidity and mortality as well as the rates of all-cause hospitalization, emergency department visits, and CAP-related hospital visits [5]. In 2019, pneumonia and influenza were the ninth leading cause of death in the United States, accounting for over 49,000 deaths [6]. Pneumonia-related deaths in patients admitted to the intensive care unit (ICU) was approximately 30%, however, with the COVID-19 pandemic caused by the novel Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), mortality has increased to 35-50% [7]. The COVID-19 pandemic has further highlighted the dangers of viral pneumonia, with over 2.7 million deaths worldwide and over 539,000 deaths in the United States as of March 24, 2021 [8,9].
With the significant global health burden that pneumonia poses, it is essential to improve therapeutic and management strategies [10]. Although there are many treatments available, including antibiotics, corticosteroids, breathing treatments, and oxygen therapy, the increasing emergence of antibiotic-resistant bacterial strains limits options for effective antibiotic use [3,10,11]. Furthermore, approximately 14-35% of hospitalized CAP patients die despite appropriate antibiotic treatments [12]. Beyond the problems associated with antibiotics, the use of corticosteroids has been controversial due to their associated adverse side effects, demonstrating the need for other therapeutic options. In this review, we summarize the most updated research and therapeutic guidelines for treating pneumonia, specifically antibiotics and mesenchymal stem cell therapies.
Although antibiotics remain the primary treatment for bacteria-induced pneumonia, many of the currently available pharmacological agents have limitations, including allergies, antibiotic resistance, inadequate penetration in lung tissues, and adverse side effects [13]. Despite improvements in clinical management of pneumonia, treatment failure rates for pneumonia remain high at 2.4%-31.0% in CAP and 30.0%-62.0% in HAP [14]. Among the many factors that contribute to treatment failures, one major cause is associated with antibacterial therapies. Antibiotic resistance, for example, makes up more than 80% of the cases in bacteria-induced HAP [14]. The acquisition of antibacterial resistance genes by ESKAPE pathogens has increased the disease burden and death rates [15]. ESKAPE pathogens are antibiotic-resistant bacteria including E. faecium, S. aureus, K. pneumoniae, A. baumannii, P. aeruginosa, and Enterobacter, that have developed resistance mechanisms against many antibiotics, including those that are used as the last line of defense [15,16]. Mechanisms of drug resistance include drug inactivation, modification of drug binding sites or targets, changes in cell permeability that reduce intracellular drug accumulation, and biofilm formation [17].
While most common CAP-causing Enterobacteriaceae are generally susceptible to typical antibiotics, a high prevalence of S. pneumoniae strains (20-40%) are resistant to macrolides [18]. Current levels of resistance to fluoroquinolones while still relatively low, continue to increase [18]. Furthermore, fluoroquinolones have been associated with adverse side effects, prompting the United States Food and Drug Administration to suggest that they be reserved for patients with no other treatment options [18,19]. High rates of treatment failure caused by inadequate antibiotic treatments have led to increased mortality and morbidity as well as longer hospital stays, highlighting the need for newer effective antibiotics [11]. These new antibiotics may address deficits in current antimicrobial drugs, with an ability to cover both typical, atypical, and resistant pathogens [7,20]. There are many approaches to antibacterial drug design, such as targeting enzymes that are essential for bacterial survival [21]. While their use in severe CAP is not yet completely understood, these novel antibiotics may offer a potential treatment option for patients with resistant pathogens (Table 1).
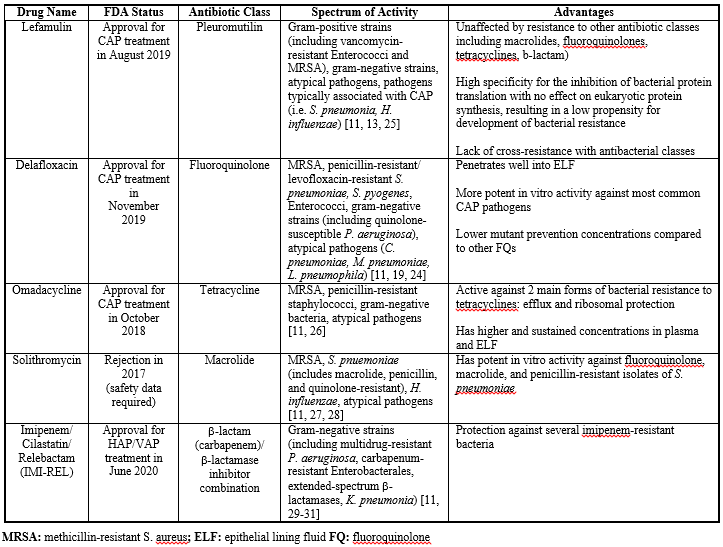
Lefamulin
Lefamulin is a pleuromutilin antibiotic that inhibits bacterial growth by binding to the peptidyl transferase center of the 50S ribosome, preventing the binding of tRNA for peptide transfer and inhibiting peptide bond formation [13,20,22]. The binding pocket of the bacterial ribosome closes around the pleuromutilin, causing an induced fit and tightening the binding pocket [13,22-24]. This unique binding mechanism is believed to be the reason for the low potential for the development of bacterial resistance and cross-resistance to other antibiotics [13, 22-24]. Lefamulin exhibits both bactericidal and bacteriostatic activity against gram-positive, fastidious gram-negative, atypical pathogens, and some gram-negative anaerobes [13,25]. It has also been shown to achieve extensive penetration and accumulation in pulmonary epithelial lining fluid [13]. These properties suggest that lefamulin could target several limitations of current existing CAP therapies.
In a multicenter randomized control phase III trial (LEAP 1), IV-to-oral lefamulin was non-inferior to IV-to-oral moxifloxacin in early clinical response (87.3% vs. 90.2% respectively, difference -2.9%, 95% CI -8.5 to 2.8) [32]. In a LEAP 2 trial, early clinical response rates were 90.8% for oral lefamulin and 90.8% for oral moxifloxacin (difference 0.1%, 1-sided 97.5% CI, -4.4% to ∞) [32]. The most frequently reported treatment-emergent adverse events were gastrointestinal, (diarrhea 12.2% in lefamulin, 1.1% in moxifloxacin; nausea 5.2% in lefamulin and 1.9% in moxifloxacin) [32]. Both studies showed that lefamulin was non-inferior to moxifloxacin and was safe and well-tolerated [32].
Lefamulin is an effective and well-tolerated agent, with availability in both oral and IV formulations to treat CAP. Patients who may benefit from lefamulin include those at higher risk of adverse events from fluoroquinolone use, those with a history of C. difficile infection, or those in settings with high prevalence of community-associated methicillin-resistant S. aureus (MRSA) [23].
Delafloxacin
Delafloxacin is an anionic fluoroquinolone with a unique structure that allows for increased intracellular penetration in bacteria, enhancing bactericidal activity in acidic conditions [33]. This property is a unique aspect of delafloxacin, as many other agents including other fluoroquinolones, macrolides, and aminoglycosides typically exhibit decreased antibacterial potency in acidic conditions [33]. Delafloxacin targets both topoisomerase IV and DNA gyrase to inhibit bacterial DNA replication [19,33,34]. This increased intracellular penetration in combination with delafloxacin's unique mechanism gives it a broad spectrum of activity against gram-positive, gram-negative, and atypical organisms, and is approved for the treatment of CAP caused by S. pneumoniae, S. aureus (methicillin-susceptible isolates only), K. pneumoniae, E. coli, P. aeruginosa, H. influenzae, H. parainfluenzae, C. pneumoniae, L. pneumophila, and M. pneumoniae [33].
In a multicenter randomized phase III clinical trial (DEFINE-CABP), delafloxacin was shown to be non-inferior to moxifloxacin (88.9% vs. 89.0% respectively, difference -0.2%, 95% CI -4.4% to 4.1%) [35]. Treatment-emergent adverse events occurred in 15.2% of the subjects in the delafloxacin group and 12.6% in the moxifloxacin group, with most events considered mild in severity [35]. Based on baseline MIC90 values, delafloxacin demonstrated 16-fold greater activity compared to moxifloxacin for gram-positive and gram-negative pathogens [35].
In a multicenter randomized phase III clinical trial (DEFINE-CABP), delafloxacin was shown to be non-inferior to moxifloxacin (88.9% vs. 89.0% respectively, difference -0.2%, 95% CI -4.4% to 4.1%) [35]. Treatment-emergent adverse events occurred in 15.2% of the subjects in the delafloxacin group and 12.6% in the moxifloxacin group, with most events considered mild in severity [35]. Based on baseline MIC90 values, delafloxacin demonstrated 16-fold greater activity compared to moxifloxacin for gram-positive and gram-negative pathogens [35].
Overall, delafloxacin is non-inferior to moxifloxacin and is effective and generally well-tolerated. In particular, it can be a potential treatment for patients with comorbidities, specifically COPD/asthma, based on improved response in these patients in the DEFINE-CABP trial [33]. Delafloxacin is a promising new antibiotic given its mild side effect profile, including a lack of association with QTc prolongation, a typical side effect of quinolones [19,36].
Omadacycline
Omadacycline is an aminomethylcycline that was created via chemical modification of minocycline and was developed to target Tet(A) and other Tet efflux genes [26,37]. The chemical modifications to its structure allow it to be active against two forms of bacterial resistance to tetracyclines: efflux and ribosomal protection. Omadacycline remains active and relatively unaffected by the presence of tetracycline efflux pumps (i.e. TetK) and ribosomal protection proteins (i.e. TetM), as well as other resistance mechanisms to other antibiotic classes [24]. It is active against staphylococci (including methicillin-resistant strains) and streptococci (including tetracycline-resistant strains). Additionally, omadacycline has a higher affinity for the 30S ribosomal subunit than tetracycline, binding to the 30S ribosome to inhibit protein synthesis [24].
In a randomized phase III clinical trial (OPTIC), omadacycline was shown to be non-inferior to moxifloxacin, with clinical success rates of 88.4% for omadacycline compared to 85.2% with moxifloxacin (difference 3.3%, 97.5% CI -2.7 to 9.3) [38]. Both treatments showed high rates of clinical success overall in patients with an identified CAP pathogen, as well as against gram-positive, gram-negative, and atypical pathogens [38]. Furthermore, there was no evidence of decreasing susceptibility to omadacycline during treatment. However, there is also a mortality imbalance in patients with CAP (2% in the omadacycline group compared to 1% in the moxifloxacin group) [38]. As the cause of the mortality imbalance has not yet been established, patients with CAP on omadacycline should be closely monitored [38]. The United States Food and Drug Administration (FDA) has required an additional active-controlled safety study in pediatric patients age 8-17 to further define omadacycline's safety and efficacy in the treatment of CAP [24,39].
In addition to its mild side effect profile, omadacycline can be used to treat patients with known hypersensitivity or intolerance to vancomycin and b-lactams, making it another potential option for treatment of CAP [26].
Solithromycin
Solithromycin is a “fourth generation” macrolide and fluoroketolide that has yet to receive FDA approval for treatment of CAP [20,40]. Solithromycin binds the 50S ribosomal subunit near the peptide exit tunnel, prematurely terminating translation and causing frameshift errors in translation [28,41]. This mechanism is considered bactericidal, however, due to its added ability to interfere with the formation of the ribosomal 50S unit, ketolides are considered bacteriostatic [41]. Furthermore, ketolides are less sensitive to macrolide efflux (mef), contributing to solithromycin’s restored activity against H. influenzae [41]. Its structure helps solithromycin to overcome macrolide resistance in addition to problems with adverse events of telithromycin [41]. In particular, solithromycin lacks a pyridine moiety which may reduce hepatic toxicity, and has fluorine at C-2, improving drug binding and enhancing activity [28, 41].
A multicenter double-blind randomized phase II study demonstrated that solithromycin has comparable efficacy and favorable safety compared to levofloxacin, with an 84.6 efficacy outcome rate of clinical success in the solithromycin group compared to 86.6% in the levofloxacin group, and early response success rates at 72.3% vs. 71.6% respectively [27]. The majority of treatment-emergent adverse events were mild-to-moderate gastrointestinal symptoms (diarrhea 7.8% in solithromycin vs. 5.9% in levofloxacin; nausea 1.6% in solithromycin vs. 10.3% in levofloxacin; vomiting 0% in solithromycin vs. 4.4% in levofloxacin) [27].
Subsequent phase III trials used moxifloxacin as the comparator. A multicenter double-blind randomized phase III trial (SOLITAIRE-ORAL) compared the efficacy and safety of oral solithromycin with oral moxifloxacin and showed that solithromycin was non-inferior to moxifloxacin in the treatment of CAP [42]. Early clinical response was achieved in 78.2% of the solithromycin group compared to the 77.9% in the moxifloxacin group (difference 0.29%, 95% CI -5.5 to 6.1) [42]. Both drugs showed similar safety profiles, with a 10% incidence of treatment-emergent adverse events in the solithromycin group compared to the 13% in the moxifloxacin group [42]. The most common adverse events were mild gastrointestinal symptoms (diarrhea 4% in solithromycin vs. 6% in moxifloxacin; nausea 4% in both groups; vomiting 2% in both groups) and nervous system symptoms (headache 4% in solithromycin vs. 3% in moxifloxacin; dizziness 2% in both groups) [42]. It was noted that overall ALT concentrations of >3 times, >5 times, and >10 times the upper limit of normal were noted in 7.2%, 2.4%, and 0.1% of patients in the solithromycin group in comparison to the 3.6%, 1.0%, and 0.2% in the moxifloxacin group [28, 42].
A second phase III trial (SOLITAIRE-IV) evaluated the safety and efficacy of IV-to-oral solithromycin and moxifloxacin, also supporting prior studies’ conclusions that solithromycin was non-inferior to moxifloxacin [43]. Early clinical response was achieved in 79.3% of the solithromycin group compared to the 79.7% in the moxifloxacin group (difference -0.46%, 95% CI -6.1 to 5.2) [43]. Adverse events were comparable between the two groups, though mostly mild/moderate infusion events led to a higher incidence of adverse events in the solithromycin group [43].
Solithromycin is an effective antibiotic regimen that offers additional advantages, including its anti-inflammatory effect and its potent activity against pathogens [40]. However, due to concerns related to hepatoxicity, the FDA has recommended further clinical studies to assess the safety profile in 9000 patients [20,28].
Imipenem/Cilastatin/Relebactam (IMI-REL)
IMI-REL is a new intravenously administered b-lactam (carbapenem)/ b-lactamase inhibitor anti-infective combination antibiotic that recently received FDA approval for use in treating HAP and ventilator-associated pneumonia (VAP) in June 2020 [30]. Imipenem is a carbapenem that inactivates penicillin-binding proteins to inhibit peptidoglycan crosslinking during cell wall synthesis, resulting in bacterial cell lysis and death [30]. It is coadministered with cilastatin, a dehydropeptidase-I inhibitor that does not have antibacterial activity and simply reduces renal metabolism [29,30]. Relebactam is a novel b-lactamase inhibitor that protects imipenem from degradation by Pseudomonas-derived cephalosporins and class A and C b-lactamases, helping to restore imipenem activity against several imipenem-resistant bacteria including P. aeruginosa and Enterobacteriaceae [29-31]. IMI-REL has a broad spectrum range in vitro, including multidrug-resistant P. aeruginosa and carbapenem-resistant Enterobacterales [29-31].
Two phase III trials of IMI-REL have been conducted to study its efficacy and safety. In a double-blind randomized phase III trial (RESTORE-IMI 1), the efficacy and safety of IMI-REL were comparable to that of imipenem/cilastatin + colistin for the treatment of hospitalized patients with hospital-acquired/ventilator-associated pneumonia, complicated intraabdominal infection, or complicated urinary tract infection caused by imipenem-nonsusceptible pathogens [44]. A favorable overall response was observed in 71% of the IMI-REL group compared to 70% of the imipenem + colistin group. Serious adverse events occurred in 10% of the IMI-REL group as opposed to 31% in the imipenem + colistin group [44]. The second double-blind randomized control phase III trial (RESTORE-IM 2) demonstrated noninferiority of IMI-REL compared to piperacillin/tazobactam in patients with HAP/VAP [45]. The favorable early clinical response was 61.0% in the IMI-REL group compared to the 55.8% in the piperacillin/tazobactam group; Day 28 all-cause mortality was 15.9% in the IMI-REL group compared to 21.3% in the piperacillin/tazobactam group (difference -5.3%, 95% CI -3.2 to 13.2) [45]. Serious adverse events occurred in 26.7% of the IMI-REL group vs. 32.0% of the piperacillin/tazobactam group [45]. Common adverse events included anemia, elevated liver enzymes, gastrointestinal symptoms (nausea, vomiting, diarrhea), and headaches [45].
The two studies demonstrate that IMI-REL is generally well-tolerated and is a viable treatment option for gram-negative HAP/VAP, including in critically ill, high-risk patients [44,45].
The official clinical practice guideline of the American Thoracic Society (ATS) and Infectious Diseases Society of America (IDTA) for the diagnosis and treatment of CAP recommends corticosteroid treatment only for patients with CAP and refractory septic shock [46]. Corticosteroid use to decrease inflammation in patients with severe CAP has been studied for decades with conflicting results [7,12]. Corticosteroids can be used as adjuvant therapy for acute respiratory distress syndrome, though use in severe viral pneumonia is controversial due to numerous negative side effects associated with it [47]. Potentially, corticosteroids may decrease cytokines to reduce inflammation and help with inadequate adrenal response in critically ill patients [48]. Because antibiotics are largely used to treat bacteria-induced pneumonia, steroids are mainly tested for the treatment of viral-induced pneumonia. Due to the controversies surrounding corticosteroid use in treating CAP, many clinical trials have been performed to evaluate the safety and efficacy of several steroids, particularly in the treatment of SARS-CoV-2 induced pneumonia (Table 2).
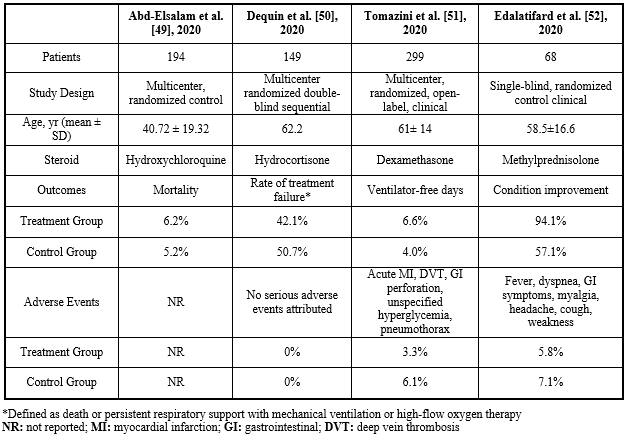
In light of the COVID-19 pandemic, several clinical trials have been conducted to determine the efficacy and safety of steroids in treating SARS-CoV-2 induced pneumonia. In a multicenter randomized control study done by Abd-Elsalam et al. evaluating the safety and efficacy of hydroxychloroquine (HCQ) with standard care in patients with COVID-19, the overall mortality did not differ between the control and experimental group (6.2% patients with HCQ + standard care vs. 5.2% patients with standard care alone) [49]. Moreover, patients in the HCQ + standard care group experienced more negatives side effects (i.e. difficulty seeing and hearing, unusual bleeding, irregular heartbeat, etc.) compared to the control group [49].
Dequin et al. conducted a clinical trial on the efficacy of low-dose hydrocortisone in patients with COVID-19 induced acute respiratory failure and found that there was no significant difference in the rate of death or persistent respiratory support with mechanical ventilation or high-flow oxygen therapy between the group treated with low-dose hydrocortisone and the control group (42.1% in the treatment vs 50.7% in the control) [50].
Tomazini et al. conducted a multicenter randomized open-label clinical trial in 41 ICUs in Brazil to determine if intravenous dexamethasone could treat SAR-CoV-2 induced acute respiratory distress syndrome (ARDS) [51]. Sequential Organ Failure Assessment (SOFA) scores (range, 0-24, with higher scores indicating greater organ dysfunction) were used to evaluate the differences [51]. At 7 days, patients in the dexamethasone treatment group had a mean SOFA score of 6.1 (95% CI, 5.5 to 6.7) in comparison to a 7.5 (95% CI, 6.9 to 8.1) in the standard care group (difference, -1.16; 95% CI, -1.94 to -0.38; P = .004) [51]. However, on day 28, 21.9% in the dexamethasone group compared to the 29.1% in the standard care group experienced secondary infections, and 3.3% vs 6.1% experienced serious adverse events [51]. This study showed that dexamethasone treatment decreases secondary infections and serious adverse events [51]. Despite its efficacy, however, it is important to note that dexamethasone is associated with many side effects, including mental depression, mood change, headache, and irregular heartbeat.
Lastly, Edalatifard et al. conducted a single-blind randomized controlled clinical trial in Iran to evaluate methylprednisolone’s ability to reduce the inflammation of the respiratory system in patients with COVID-19 [52]. There was a higher incidence of improvement in the methylprednisolone treatment group than in the standard care group (94.1% vs. 57.1%) [52]. Furthermore, the mortality rate was significantly lower in the methylprednisolone group (5.9% vs. 42.9%; p < 0>
Based on the results of the multiple clinical trials conducted, most steroids were not very effective in treating pneumonia. Although some steroids may have shown efficacy in treating pneumonia, they are also associated with many negative adverse events, prompting the ATS/IDTA to recommend against routine corticosteroid use in treating CAP and severe influenza pneumonia [46]. Given these adverse events and recommendations, several studies have been conducted evaluating the use of alternative therapies in place of corticosteroids.
Mesenchymal stem cells (MSCs) are adult multipotent stem cells found in bone marrow and have potent immunomodulatory properties to suppress the pro-inflammatory processes in the lungs, though its mechanism of action is not yet fully understood [53,54]. Recent studies, however, have identified several mechanisms through which MSC treatments can promote tissue repair, including mitochondrial transfer, exosome transfer, and paracrine secretions. Mitochondrial transfer from MSCs to innate immune cells has been shown to enhance phagocytic activity [53]. Additionally, MSC paracrine activity appear to module immune responses and promote cell survival. MSCs secrete several factors that support survival, including growth factors, cytokines, and extracellular matrix, which theoretically can rescue injured cells to reduce tissue damage and accelerate tissue repair [54]. Subsequent release of soluble factors after MSC activation can lead to the differentiation, proliferation, and activation of immune cells including T cells, B cells, macrophages, and mast cells, inhibiting local inflammation [55,56]. Lastly, MSCs have played a role in maintaining tissue homeostasis and in modulating inflammatory disease [57]. Although the mechanisms of MSC treatments are still not yet fully understood, MSC treatments may have a specific therapeutic potential and safety profile in the treatment of pneumonia that may be used in place of corticosteroid therapies [55].
The first line of treatment for bacteria-induced pneumonia is the empiric prescription of antibiotics, while stem cell therapies are being considered as a replacement for corticosteroid treatments. Gupta et al. conducted a study using a mouse model of gram-negative pneumonia to evaluate the efficacy of MSCs [58]. MSCs could reduce lung injury and increase survival (55% in the MSC group vs. 8% in the 3T3 control and 0% in the PBS control group). Furthermore, MSCs were noted to enhance bacterial clearance in the alveolar space as early as 4 hours following administration and were still able to retain their classic immunosuppressive properties [58]. Moreover, MSCs significantly upregulated their production of lipocalin 2, an innate immune protein used to prevent the growth and spread of microorganisms [58,59]. The same research group also conducted a study to test the effect of human MSCs derived from bone marrow on the bacterial growth of gram-negative (E. coli and P. aeruginosa) and gram-positive (S. aureus) bacteria and found that MSCs directly inhibited bacterial growth [59]. While Gupta et. al concluded that MSCs could be beneficial in bacteria-induced pneumonia, it has not yet been clinically tested in humans [58,59]. Clinical trials would be required to determine the efficacy and safety of MSCs in treating bacteria-induced pneumonia in humans.
MSCs have the potential to treat virus-induced pneumonia. Chen et al. demonstrated that MSC transplantation in treating H7N9 virus-induced acute respiratory distress syndrome (ARDS) was both safe and effective, lowering the mortality rate in the experimental group, compared with the control group (17.6% vs. 54.5%) [60]. Furthermore, 85% of patients showed significant improvement at their 3-month follow-up visit [60]. MSC transplantation also did not show any significant side effects [60]. This study suggests that MSCs significantly improved the survival rate of H7N9-induced ARDS. This evidence of the potential use MSCs in treating virus-induced pneumonia is important, as their mechanisms of action may be similar for many other different types of viral infections.
A majority of the studies evaluating the efficacy and safety of MSCs have been performed on virus-induced pneumonia. While the efficacy and safety of MSCs in treating bacteria-induced pneumonia have not yet been determined in humans, there have been numerous clinical trials performed to test the safety and efficacy of MSCs in treating virus-induced pneumonia (Table 3).
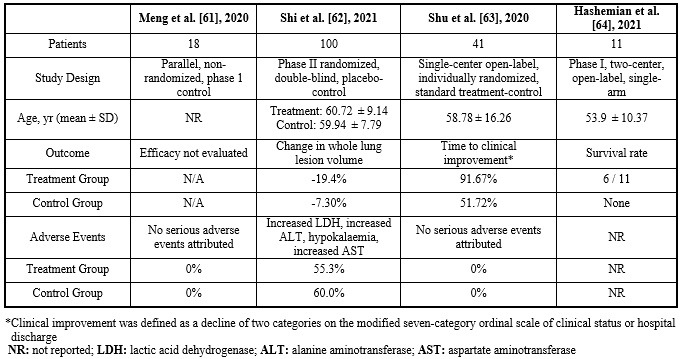
Meng et al. conducted a parallel non-randomized phase I clinical trial evaluating the safety of human umbilical cord-derived mesenchymal stem cell (UC-MSCs) infusions on patients with moderate-to-severe COVID-19 pulmonary disease [61]. No serious UC-MSCs infusion-associated adverse events were observed and all patients had recovered and were discharged, demonstrating that intravenous UC-MSCs infusions are safe [61].
Two individual clinical studies were conducted testing both the efficacy and the safety of UC-MSCs in treating COVID-19-induced pneumonia. Shi et al. demonstrated that the administration of UC-MSCs improved whole lung lesion volume from baseline to day 28 compared to the placebo group (the median difference -13.31%, 95% CI -29.14% to 2.13%, P = 0.080) [62]. UC-MSCs also significantly reduced the proportions of solid component lesion volume (median difference -15.45%; 95% CI -30.82% to 0.39%; P = 0.043). Moreover, the incidence of adverse events was similar between the treatment group and the placebo group, indicating that UC-MSCs were not only effective, but also did not have severe side effects and were safe to use [62]. Similarly, Shu et al. found that patients in the UC-MSC had a shorter time to clinical improvement in comparison with the control group (median 9.0 days vs. 14.0 days respectively, P = 0.006) [63]. Furthermore, all of the patients in the treatment group had no adverse reactions (rash, allergic reaction, and febrile reaction) [63]. Both studies done by Shi et al. and Shu et al. demonstrate that the administration of UC-MSCs in the treatment of COVID-19 induced pneumonia was effective and safe.
Hashemian et al. also conducted a clinical trial to evaluate the safety, feasibility, and tolerability of the multiple infusions of high dose MSCs derived from the placenta and umbilical cord in treating COVID-19 induced pneumonia [64]. No serious adverse events were reported within 24-48 hours of cell infusions, and reduced dyspnea and increased oxygen saturation (SpO2) levels were observed within 48-96 hours after the first infusion in 7 out of 11 patients [64]. Overall, six patients survived with significant reductions in serum levels of tumor necrosis factor-alpha (TNF-α; P < 0>
In summary, MSC treatments are safe and effective in treating COVID-19 induced pneumonia, making them an ideal potential replacement for corticosteroid treatments for COVID-19 patients. Recently, the FDA has given conditional approval for use of stem cell treatments on severe COVID-19 patients under “expanded access compassionate use” [61,62]. However, further clinical trials may be necessary to further the establish efficacy and safety of MSC treatments, not only in treating COVID-19 patients but also in treating other virus-induced pneumonia, especially if they are to be considered a replacement for corticosteroids.
Because both MSCs and novel antibiotics are promising therapies for the treatment of pneumonia respectively, a few studies have been conducted to determine the efficacy and safety of combined stem cell and antibiotic treatments.
Kong et al. conducted a study testing the combined treatment of antibiotic linezolid and human MSCs (hUMSCs) on a rabbit model with MRSA-infected pneumonia [65]. Linezolid monotherapy (50 mg/kg for two times/day) resulted in improvement of body weight, chest imaging, bronchoscopic manifestations, histological parameters, and IL-10 concentration in plasma (P < 0>
Combination treatment with both stem cells and linezolid showed significantly improved therapeutic effects in comparison to linezolid treatment alone [65]. Further clinical trials, however, are needed to show that this combination treatment is also effective and safe in treating pneumonia in humans.
Although MSCs can be isolated from a variety of sources, like bone marrow, adipose tissue, umbilical cord, dental pulp stem cells, and endometrial MSCs, the availability of MSCs for the treatment of disease is still very low [66]. The eligibility requirements to donate MSCs are limited based on gender, BMI, donor site, age, and diseases [66]. Furthermore, the isolation procedures of MSCs are also very challenging. Even after successful isolation, the number of cells from the primary culture is often insufficient for clinical application, requiring cell expansion [66]. Due to the challenging manufacturing processes and limited availability of MSCs, the current cost of MSCs is quite expensive, varying from $15,000 to $30,000 per 1–5 million cGMP‐MSCs per kilogram [66]. Improvements in cell expansion technologies to make MSC treatments more readily available and cost-effective need to continue to develop for MSC treatments to become a viable treatment option for pneumonia [67].
Pneumonia continues to remain an important infection due to its impact on patient outcomes, especially amongst young children, the elderly, and immunocompromised patients. The availability of new antibiotics offers an opportunity for the treatment of antibiotic-resistant pathogens associated with both CAP and HAP. These new drugs have a broad spectrum of activity against pathogens, including multidrug-resistant strains that pose a major threat to clinical practice given the limited therapeutic options. Moreover, in addition to having similar safety and efficacy profiles as older drugs, several of these newer drugs have structural characteristics that allow for a decreased propensity in the development of bacterial resistance.
In addition to novel antibiotics, the potential use of stem cell therapies in place of corticosteroid treatments may offer an improvement in patient outcomes. Novel stem cell therapies, especially human UC-MSCs, showed efficacy and safety on COVID-19 induced pneumonia. However, further research and clinical trials are needed to demonstrate the efficacy and safety of UC-MSCs in the treatment of other virus-induced pneumonia beyond COVID-19.
The combined treatment of both stem cells and antibiotics in pneumonia in a rabbit model showed significantly increased efficacy in comparison to antibiotic treatment alone, presenting a possible route for a novel strategy in treating pneumonia, though additional future studies are necessary before clinical implementation.
While pneumonia remains a major disease of concern, having newer approved antibiotics as well as novel therapies such as stem cell treatments in the pipeline offers clinicians more options to effectively treat pneumonia.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
